
Factors Related to Depression among Older People Living in Homes for the Aged of the Western Part of Thailand
Geriatric or late life depression is one of the significant mental health issues for older people (Bolger, 2005) because it may link to health status and well-being of older people (Rodriguez‐Blazquez et al., 2012). This is particularly true of older people living in homes for the aged which provided care at the minimum requirement by public or government sector for the poor, those who have been neglected or abused, or who have no family caregivers to look after them. The prevalence of depression among people living in nursing homes and homes for the aged is about 25-42% (Somporn, 2011; Suwattanakoop, 2013; Wongpakaran & Wongpakaran, 2012). Unfortunately, most health care professionals usually under-recognize and under-treat depression, because late life depression is complex and difficult to diagnose. As a result, under-recognition and under-treatment may lead to poor quality of life and inaccessibility to proper care for older people suffering from depression. Consequently, suicide may impact them later (Bolger, 2005). Risk factors which are the leading causes of late life depression are physical impairment or comorbidity (such as chronic illnesses, pain) (Piboon et al., 2012), bereavement, adverse life events, loneliness, and social isolation (Bolger, 2005). Furthermore, some studies (Piboon et al., 2012) mentioned that getting old, being female, health status, greater number of chronic illnesses or, functional status such as Activities of Daily Living (Jitaree, 2012), social support, grief and loss experience were associated with depression. Some previous studies demonstrated the issues and problems of depression in nursing homes located in many cities in Thailand such as Bangkok (Somporn, 2011), Chiang Mai (Suwattanakoop, 2013; Wongpakaran & Wongpakaran, 2012) and Nakhonratchasima (Satra, 1988). However, a study that can illustrate depression issues among older people living in homes for the aged in the western part of Thailand, including Suphanburi, Kanchanaburi, Nakhonpathom, Samutsakhon, Samutsongkram, Ratchaburi, Pethchaburi, and Prachuebkirikhun province, which are different from the areas looked at in previous studies in terms of geography and culture, is required because of a lack of a prevalence study in this part of Thailand. In addition, the earlier study in Bangkok was affected by the big flood in Thailand during 2012. Most studies advised that older people living in homes for the aged tend to have a higher prevalence of depression than those living in the community (Somporn, 2011; Wongpakaran & Wongpakaran, 2012). However, studies of factors related to depression in homes for the aged in this area are scarce. Therefore, the researchers would like to investigate the prevalence of depression and associated factors of depression to help understanding and develop an appropriate depression intervention program for older people living in homes for the aged in the western part of Thailand in the future.
Objectives
There were two main purposes of this study:
-
to examine the depression rate among older people living in homes for the aged of the western part of Thailand
-
to investigate the correlation between selected factors – gender, age, income, perceived health status, number of chronic illnesses, family relationship, recent grief and loss experience, activities of daily living – and depression among older people, living in homes for the aged in the western part of Thailand.
Methods
A correlation study was used.
Population and Sample
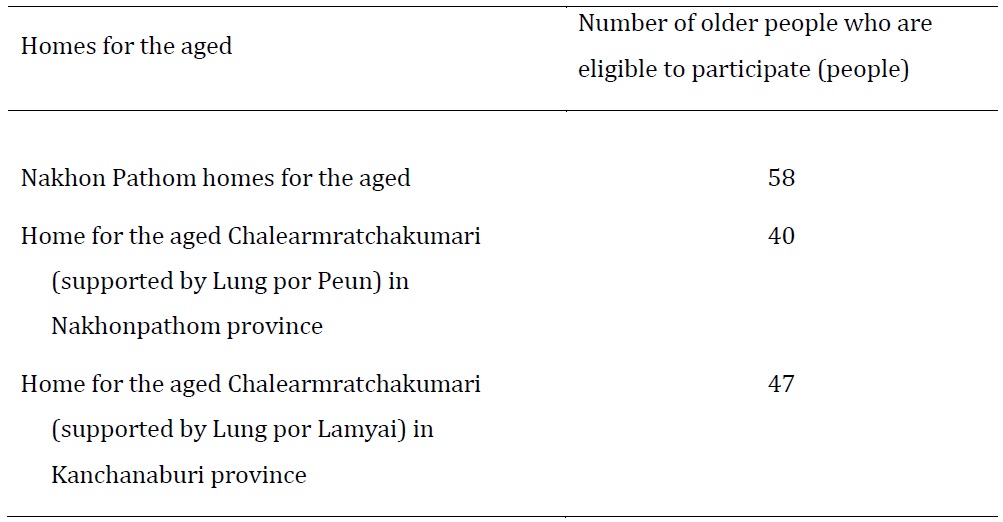
Population of this study. Based on a survey on the number of older people living in three public homes for the aged in the western part of Thailand, 145 older people who live in three public homes for the aged located in the western part of Thailand as presented in Table 1 were eligible to complete the survey.

Sample. One-hundred-seven older people living in two homes for the aged in the western part of Thailand were recruited to this study using cluster sampling. The two homes for the aged, where were located in Kanchanaburi and Nakhonpathom province, were selected.
Measurement Tools
There were three questionnaires, including:
1. Personal characteristics include gender, age, income, marital status, perceived health status, number of chronic illnesses, family relationship, and recent grief and loss experience. These questions were developed by the researchers, and the quality of questions, including validity and reliability were examined as follows:
Content validity was examined by asking 3 experts who are specializing in psychiatric nursing or measurement tool development to check the validity. Then the researchers refined the questions based on the suggestion of the experts. The reliability of personal characteristics equated to 0.72.The low reliability may due to the different aspects of questions.
2. The Barthel activity of daily living index (BADL) was well developed by Mahoney & Barthel (1965) and commonly used in studies of older people. The BADL includes 10 activities of daily living: feeding, grooming, transferring, toilet use, mobility, dressing, stairs, bathing, bowels, and bladder. Each activity can be categorized as levels of dependences. For example, 0 equates to fully dependent, 1 equates to partially dependent, and 2 equates to independent. Ranges of BADL scores were 0-20, the higher score means independent, the lower score means dependent. This study used the criteria of the Department of Health, the Ministry of Public Health to report and categorize the activities of daily living of older people into three groups: ≥12 scores means independence or well elder group
-
≥5-11 scores means partial independence or home bound
-
0-4 scores means fully dependent or bed bound group.
These above criteria were used to help readers to understand the context of older people living in homes for the aged in the western part of Thailand only. Therefore, the actual scores were used to analyze the correlation study.
The researchers did not examine the content validity of BADL because it was well developed and commonly used in the older people study in Thailand. The reliability equated to 0.95.
3. The Thai Geriatric Depression Scale (TGDS) was developed by Train the Brain Forum (1994) about depressed emotions during the previous week. This self-report questionnaire requires yes or no answer for 30 items. The range of scores was 0-30. Higher scores indicate a greater likelihood that someone is depressed. The criteria to interpret TGDS score were:
-
0-12 score refers to normal condition
-
13-18 scores refers to mild depression
-
19-24 scores refers to moderate depression
-
25-30 scores refers to severe depression
These criteria will be used in the same way as the BADL. The reliability of TGDS was 0.93.
Data Collection
After getting approval from the ethics committee from Boromarajonani College of Nursing, Chakriraj, the researchers collected data from older people who agreed freely to participate in this study after understanding all protocols. Structured interviews of about 30-45 minutes based on the questionnaires were used as the technique for this data collection. If any issues or problems with the participants had arisen, the researchers would have assessed the participants’ readiness and agreement immediately. If an interviewee became distressed, the researchers would have stopped the interview.
Data Analysis
Descriptive statistics such as percentages, medians, and Spearman’s rank correlation were used for data analyzing because the data had a non-normal distribution.
Results and Discussion
Personal Characteristics
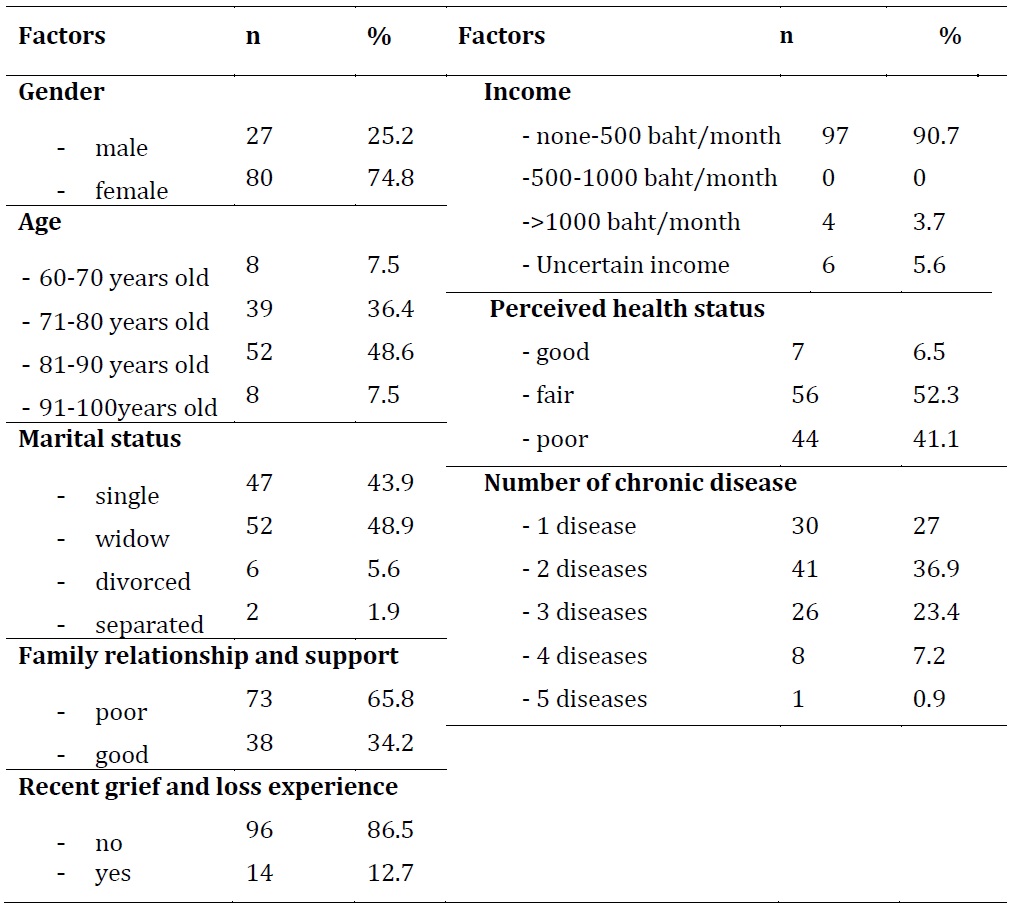
The most common characteristics were female (74.8%), 81-90 years old (48.6%), widowed (48.9%), poor family relationships and support (65.8%), no recent experience of grief and loss (86.5%), fair health status (52.2%), two chronic illnesses (36.9%). Furthermore, most of them have an income of less than 500 baht/month, as shown in Table 1.

Activities of Daily Living
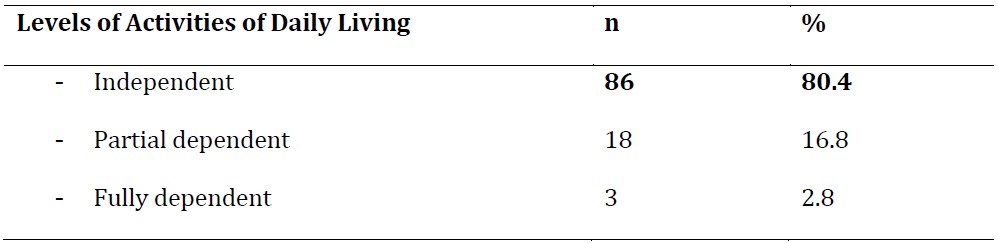
Participants were independent (80.4%), partially dependent (16.8%) and fully dependent (2.8%). Details are shown in table 2.

Depression
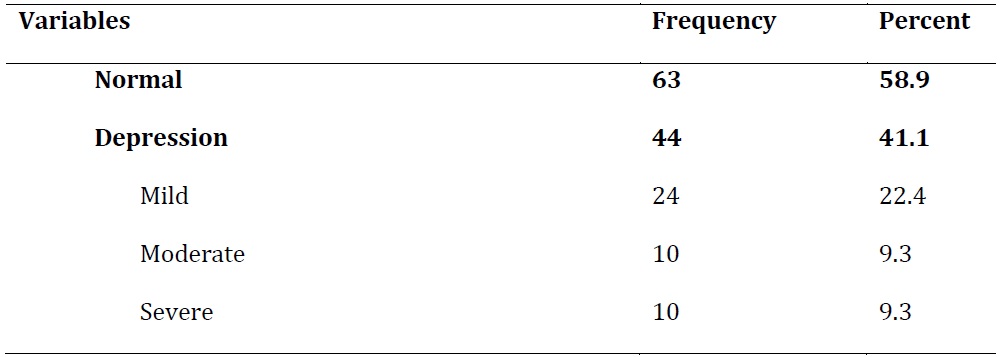
The results revealed that nearly half (41.1%) of the older people interviewed suffered from depression, whereas, the older people with normal condition was 58.9%. Most of them suffered from mild depression (22.4%) as shown in table 3.

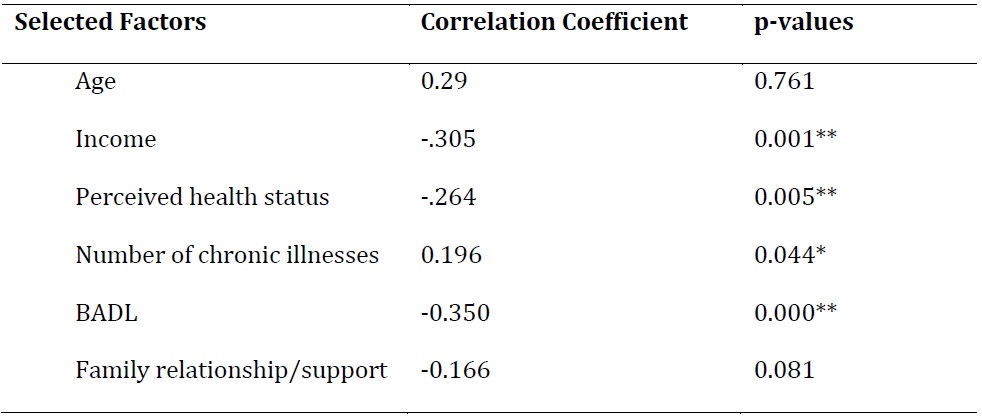
Correlation between selected factors and depression
Income, perceived health status, and BADL were significantly negatively associated with TGDS scores at p<0.01; whereas, the number of chronic diseases was significantly positively associated with depression at p<0.05, as shown in Table 4.
However, age, and family relationship/support were not significantly associated with TGDS scores, as shown in Table 4. Gender and grief and loss experience were not significantly associated with TGDS scores using Mann-Whitney U test as shown in Table 5.


Discussion
The results showed that about 41.1% of older people living in homes for the aged in western Thailand suffer from depression, which was congruent with previous research (Somporn, 2011) that found that the prevalence of mild and severe depression of older people living in Ban Bang Kae, a home for the aged in Bangkok, Thailand after flooding, was about 40%. However, this prevalence in Thailand was higher than those in Dutch aged care facilities, which found only 13.6% (Boorsma et al., 2012) and 32% in Norwegian nursing homes (Drageset et al., 2013). The higher rate may be caused by an underrecognition and under-treatment of depression in Thai older people who live in rural areas. All homes for the aged in the western part of Thailand that were included in this study were located in the rural part where there is limited access to depression screening and treatment.
Additionally, the prevalence of depression among people living in homes for the aged in the western part of Thailand may be greater than those living in the community in Nonthaburi, where 15.3% of residents were found to have depression (Poungrod, 2015). This phenomenon may be due to most participants lack of family support or stressful events in life when living in nursing homes which are congruent with Piboon’s study (2012).
Interestingly, income was negatively associated with depression. This result is also congruent with Napa Poungrod’s study (2015), which revealed that inadequate income may lead to depression among older people living in community. Furthermore, chronic illnesses and perceived health status were significantly related to depression; this phenomenon may also be the same trend with those living in community dwelling based on Napa Poungrod’s study (2015).
Furthermore, the BADL, being negatively associated with depression were found in this study and previous studies (Drageset et al., 2011; Karp et al., 2009).
However, age, gender, and family relationship/support, were not significantly related to depression, which may be caused by the similar characteristics of participants or a lack of equal number of participants in each group themselves. Therefore, it may lead to a lack of association.
Conclusion and Recommendation
Results of this research the correlation may guide the treatment and practices in the future. For example, the officers or health care providers in homes for the aged should encourage older people to be independent, improve their perceived health status, increase health promoting behaviors to prevent or delay chronic illnesses, or increase older’s people incomes by promoting appropriate occupations.
Biographical Note
Sirikul Karuncharernpanit is an instructor and registered nurse at Boromarajonani College of Nursing, Chakriraj, Ratchaburi, Thailand. She can be reached by email at ksiriku@hotmail.com